Benefits of peer support: What can the data tell us?
The availability of peer support services has skyrocketed in recent years and is expected to continue to grow, in part from a focused and determined peer advocacy movement. While many peers and service users attest to the benefits of peer support services in enhancing recovery and wellness, the research literature is dominated by mixed reports about the effectiveness of peer support services. However, we argue this should not be taken as evidence that peer support services are not effective for several reasons which we outline below.
First, several large, well-designed studies of peer-facilitated recovery self-management interventions have shown benefits over comparison conditions. Cook and colleagues conducted an outpatient 8-week wait-list control study of a peer-facilitated Wellness Recovery Action Plan (WRAP) group intervention with a total of 555 individuals with serious mental health conditions (1, 2). At the end of treatment and 6-month follow-up, WRAP participants showed greater improvements over the intervention compared to wait-list period in mental health symptoms, self-perceived recovery, hopefulness, quality of life, self-advocacy, personal confidence, and goal orientation. Another study by this group evaluated the peer-facilitated Building Recovery of Individual Dreams and Goals through Education and Support (BRIDGES) outpatient 8-week group intervention, using a wait-list control design, and included a total of 428 individuals with serious mental health conditions (3). Participants showed greater improvements over the intervention period in self-perceived recovery and some measures of hopefulness at the end of treatment and 6-month follow-up. Johnson and colleagues randomized 441 individuals who were exiting care from a mental health crisis team to receive either 10 individual sessions with a peer in the community focused on completing exercises in a personal recovery workbook or were mailed the recovery workbook without peer support (4). Participants in the peer-facilitated self-management intervention had lower rates of hospital readmission at one year and reported greater satisfaction with their mental health care services compared to the control group (see Figure 1).
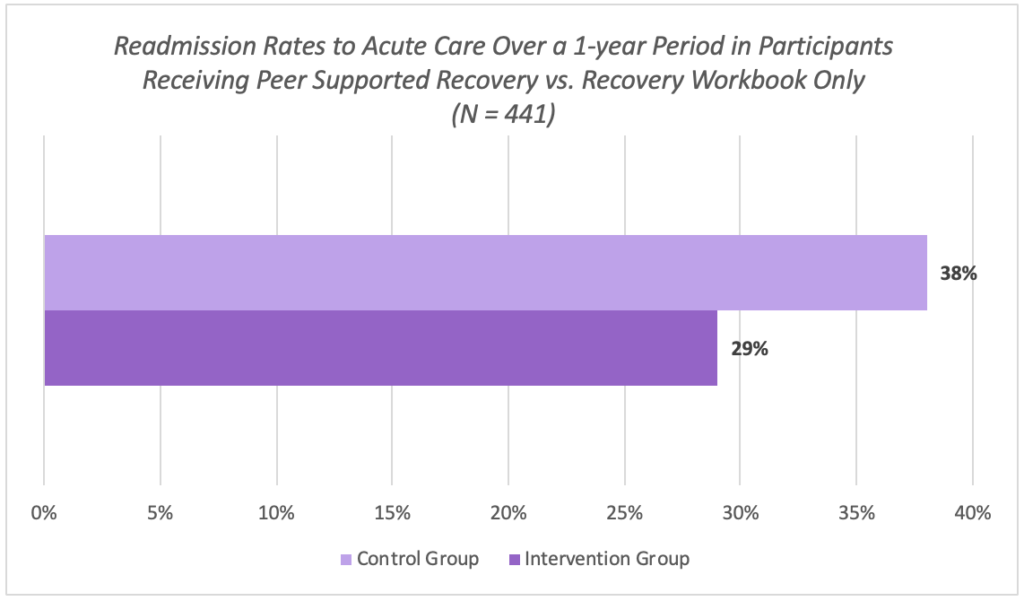
Figure 1. Hospital readmission rates at one year
Secondly, peers offer a range of services and the range of how peer services are implemented in the real-world does not lend itself to gold-standard research designs, such as a randomized controlled trials of narrowly defined peer-facilitated self-management interventions. In practice, the type of peer support provided can look very different across programs, peers, and service users. One program may train peers to support recovery goals identified in clinical care (e.g., meet up at a coffee shop as pleasant event to decrease depression), while in another setting peers may provide valuable support that is independent from clinical care (e.g., assistance with finding a new apartment). Some researchers have emphasized the need for more comprehensive assessment of the impact of peers working across diverse roles, populations, and venues outside of traditional healthcare settings that may be better in line and welcoming of the values and principles of peer support (5).
Thirdly, little is known about the mechanisms by which peer support brings about change. One way to explore this might be to evaluate differences in service users experience of and outcomes from interventions delivered by people with lived experience compared to these same interventions delivered by individuals who do not have lived experience. It may also be of interest to identify the benefits of matching peers based on background factors, life experiences and/or goals. For example, a peer supporter who has successfully quit smoking may perhaps bring more added value to a peer-led intervention for smoking cessation that a peer who never smoked or continues to smoke.
We do agree that a thoughtful approach to future research on peer support is needed, in part to inform training and supervision models and to help clarify peer roles. Research can be used to improve existing programs and guide the expansion of peer support services to new environments and service users. Hopefully future research will better assess system-level impact of peer support programs and strategies to better support and fully integrate peers in existing systems of care.
Diana Arntz, PhD
Research Fellow, MGH COE
References
- Cook, J.A., Copeland, M.E., Floyd, C.B., et al: (2012a). A randomized controlled trial of effects of Wellness Recovery Action Planning on depression, anxiety, and recovery. Psychiatric Services, 63, 541–547.
- Cook, J.A., Copeland, M.E., Jonikas, J.A., et al. (2012b). Results of a randomized controlled trial of mental illness self-management using Wellness Recovery Action Planning. Schizophrenia Bulletin, 38, 881–891.
- Cook, J. A., Steigman, P., Picket, S., Diehl, S., Fox, A., Shipley, P., MacFarlane, R., Grey, D. D., & Burke-Miller, J. K. (2012). Randomized controlled trial of peer-led recovery education using Building Recovery of Individual Dreams and Goals through Education and Support (BRIDGES). Schizophrenia Research, 136, 36-42.
- Johnson, S., Lamb, D., Marston, L., Osborn, D., Mason, O., Henderson, C., … Lloyd-Evans, B. (2018). Peer-supported self- management for people discharged from a mental health crisis team: A randomised controlled trial. The Lancet, 392(10145), 409–418.
- Gillard, S. (2019). Peer support in mental health services: where is the research taking us, and do we want to go there? Journal of Mental Health, 28 (4), 341-344.